Toe Deformities – Mallet, Hammer, Claw and Overlapping 5th Toe
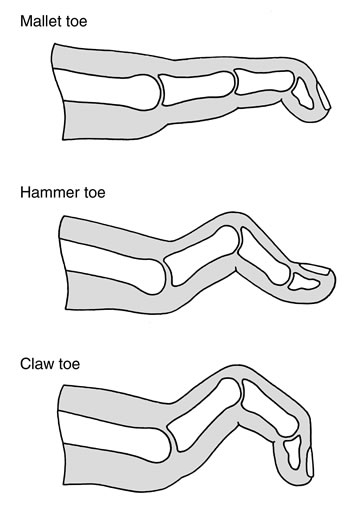
A mallet toe is a flexion deformity of the distal inter phalangeal joint of a toe. The deformity can be fixed or mobile. In the first instance consideration should be given to conservative treatment with padding, taping and orthotics. In the mobile deformity if conservative measures have failed then a tenotomy of the FDL tendon can be performed. In a fixed or recurrent deformity then the treatment of choice is a fusion of the distal inter phalangeal joint using a K-wire.
A hammer toe is a flexion deformity of the proximal inter phalangeal joint of the toe. Again the deformity can be fixed or mobile. Conservative treatment again consists of padding, taping and orthotics. Should these fail then surgery may be indicated. In the mobile deformity a flexor to extensor transfer has been described. In situations where there is a recurrent or fixed deformity then a fusion of the proximal inter phalangeal joint is usually performed.
Claw toe is a flexion deformity of the proximal inter phalangeal joint and the distal inter phalangeal joint of a toe together with hyper extension of the metatarso-phalangeal joint. If bilateral and severe in nature it is important to consider an underlying predisposing cause such as a neurological abnormality. Treatment again is conservative first with accommodative shoe wear, padding, taping and orthotics. If symptoms persist then a number of surgical options have been described. If the deformity is mobile again a flexor to extensor transfer has been described combined with a release of the metatarso-phalangeal joint and a lengthening of the extensor tendon. In a fixed deformity patients will often require a fusion of the proximal inter phalangeal joint. In severe deformities this may need to be combined with a shortening osteotomy of the metatarsal.
The overlapping 5th toe deformity is a common congenital abnormality. Although the condition can often be managed with accommodative shoe wear the toe may still become painful due to pressure effects. In these instances a soft tissue release of the metatarso-phalangeal joint together with a transfer of the extensor digitoroum longus tendon in severe cases can provide good correction of the deformity.