Flat Feet – Pes Planus
Pes planus is a term used to describe flattening of the medial longitudinal arch. In the child pes planus can be broadly divided into 2 groups – physiological and non-physiological. All infants have flat feet and in the majority an arch will develop by the age of 6 years. If a child is asked to stand on tiptoes the arch should reform and the heel should move into varus. Passive dorsiflexion of the great toe also reforms the arch in a physiological flat foot.
Non-physiological flat foot can be caused by CVT, paralytic conditions(cerebal palsy, spina bifida), generalised ligamentous laxity, tight Achilles tendon, tarsal coalition and sub-talar irritability (juvenile chronic arthritis, sub-talar arthritis, osteoid osteoma).
A peroneal spastic flat foot is a term used to describe a rigid painful flat foot. The classic description refers to patients with a tarsal coalition although irritability of the sub-talar joint caused by septic arthritis, juvenile chronic arthritis, and an osteoid osteoma have also been described. Tarsal coalition usually presents in children between the ages of 10 to 14 years. The commonest forms of tarsal coalition are calcaneo-navicular and talocalcaneal.
Tarsal coalition results from a failure of segmentation. The cartilaginous bar is thought to ossify around the time of presentation. The ossification process is thought to lead to a loss of mobility and subsequent pain. Not all patients with a tarsal coalition however will develop pain and stiffness. A calcaneo-navicular bar can often be diagnosed on an oblique xray.
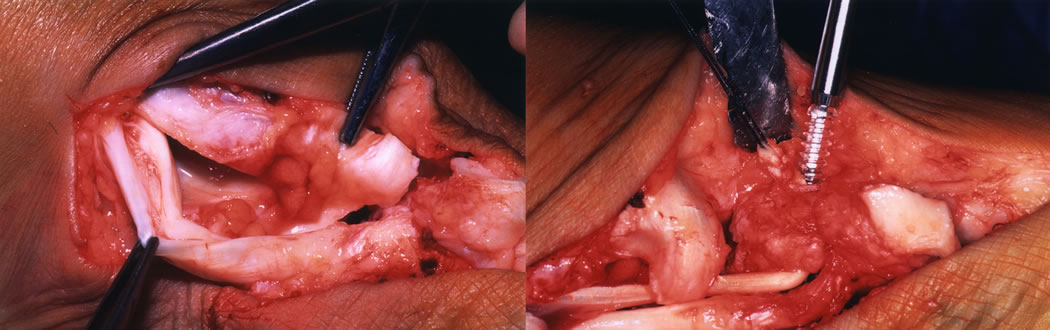
Talo-calcaneal and other forms of coalition require further imaging such as an MRI scan. Treatment depends on the severity of symptoms. In mild cases orthotics may suffice. In acutely symptomatic cases a short period of immobilisation can be helpful. Persistently painful cases often require surgery. Resection of a calcaneo-navicular bar often produces good results. The operation is performed through an Oilier type incision. The EDB is transferred into the defect following resection of the bar. Results following resection of talo-calcaneal coalitions are less predictable. The bar is usually medially placed. There may be associated deformity of the sub-talar joint or degenerative changes leading to poorer results. In the mature foot a triple arthrodesis can be used to realign the foot and improve pain.
In the adult the acquired flat foot deformity usually results from a rupture of the tibialis posterior tendon, degenerative changes within the sub-talar joint, or in association with inflammatory arthropathies classically rheumatoid arthritis.Following a rupture of the posterior tibial tendon a number of surgical options exist if non-operative treatment with orthotics fails. These include an FDL transfer and medial heel shift if the deformity is flexible. Where a fixed deformity or significant arthrosis exists a fusion is usually indicated either of the sub-talar joint or a triple fusion.