Heel Pain (Plantar Fasciitis)
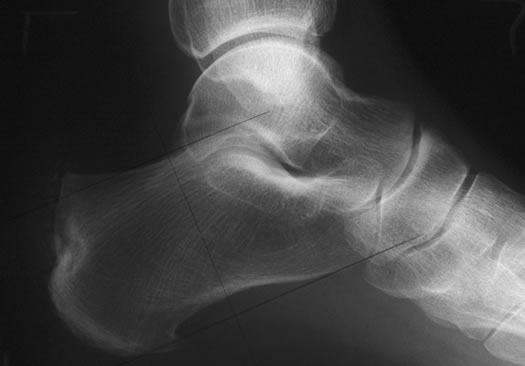
Heel pain can be broadly divided into sub-calcaneal and superior. The commonest cause of sub-calcaneal pain is plantar fasciitis. Plantar fasciitis is inflammation of the origin of the plantar fascia. The plantar fascia is a fibrous band originating from the plantar medial tubercle of the calcaneus extending to the plantar plates of the metatarso-phalangeal joints. Micro tears of the origin plantar fascia lead to chronic inflammation. There are many causes of plantar fasciitis. It is most common in patients in the age range 40 to 70 years and is more common in women than men. It is also more common in athletes and sports people. Patients complain of a gradual onset of pain around the plantar medial aspect of the heel. Symptoms are usually worst first thing in the morning. X-rays may reveal a plantar spur. Although the incidence of heel pain is higher in patients with a plantar spur many patients with plantar fasciitis have no radiological evidence of a spur.
Other causes of plantar heel pain include atrophy of the fat pad and an entrapment neuropathy of the first branch of the lateral plantar nerve. Structural causes such as a stress fracture of the os calcis should also be considered. The commonest cause of superior heel pain is an insertional Achilles tendonitis. This is often associated with a retro calcaneal bursitis and a prominent Haglund deformity. In many instances symptoms result from a change in shoe wear or level of sporting activity. Non-operative treatment including activity modification, antiinflammatories, physiotherapy and orthotics will resolve most cases. In persisting cases however, surgery may be indicated. This consists of resection of any inflamed paratenon, debridement of any degenerate tendon and resection of a prominent Haglund deformity. As well as the obvious mechanical causes of heel pain it is important to consider metabolic, inflammatory and bone disorders such as gout, hyper lipidaemias, diabetes, hypothyroidism, myeloma and Paget’s disease, all of which can present with heel pain.
The treatment of plantar fasciitis initially is conservative consisting of physiotherapy, orthotics, anti-inflammatories and modification of activity. Should the symptoms continue then a steroid injection can be of some benefit. Atrophy of the heel pad can occur following a steroid injection and patients must be warned of this. Overall approximately 80-90% of patients will see an improvement in their symptoms over a 12 month period with conservative treatment alone. Should conservative measures fail then a surgical release of the plantar fascia can be considered.